Marco Battista, Scientific Institute San Raffaele Hospital, Milan, Italy
A 70-year-old woman with a history of glaucoma since 2001 presents with a sudden decline in vision.
Although her intraocular pressure (IOP) remained well controlled with topical therapy, progression of visual field (VF) damage was noted in January 2023 (figure 1). This coincided with the diagnosis of vascular encephalopathy, followed by a revised systemic evaluation and the initiation of a more intensive anticoagulant and antihypertensive regimen.
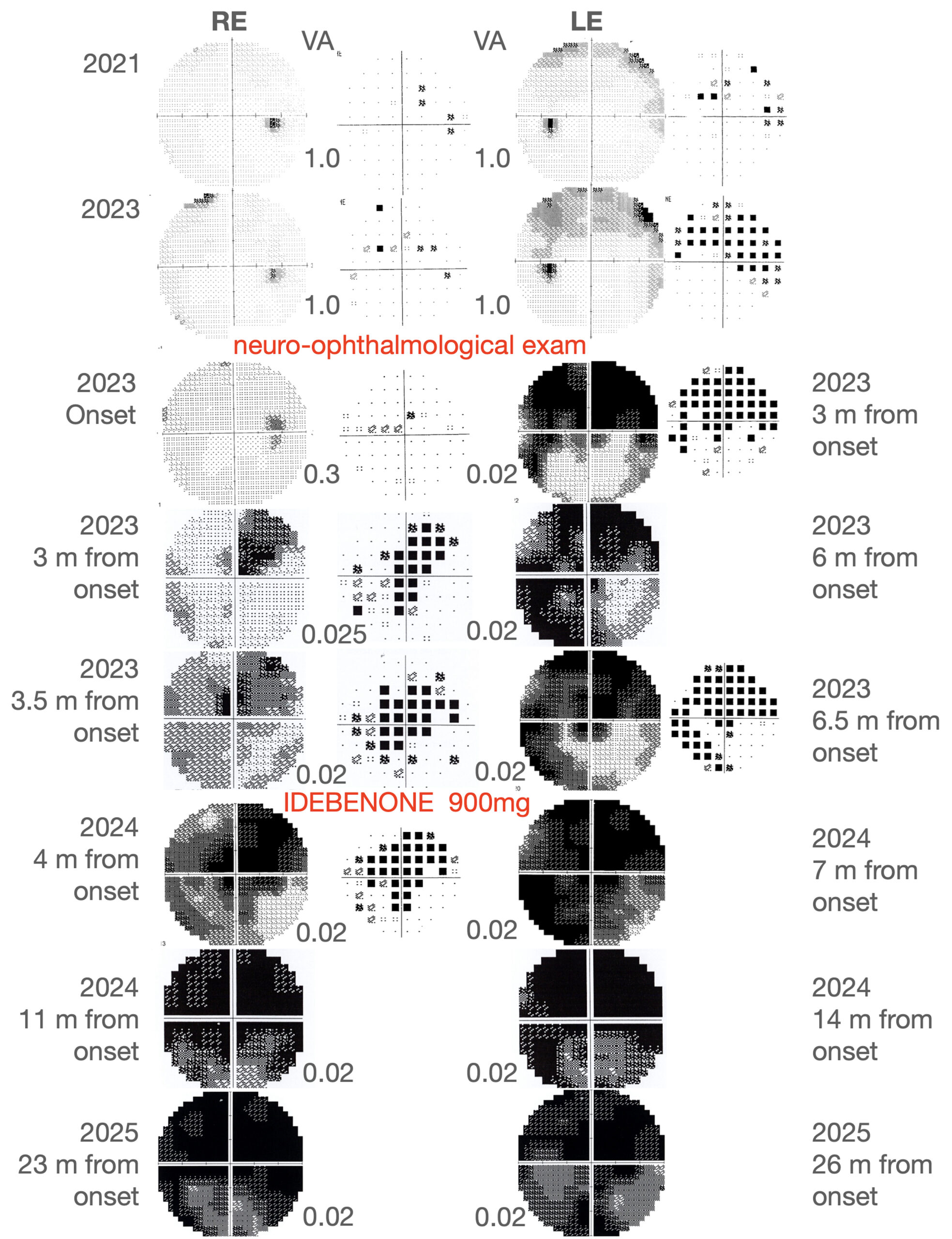
Figure 1. Visual field progression. Visual field examination in the right (OD) and left (OS) eye at different timepoints. The visual field impairment in the OS was firstly detected in the 2023 and was considered a sign of progression of the known glaucoma. At the neuro-ophthalmologic examination, the visual defect appeared deeply worsened in the superior field in the OS with only a slight paracentral involvement of the OD. Through the 2023, the OD demonstrated a faster progression of the visual field impairment, reaching a central scotoma configuration, even though also the scotoma in the OS widened. The decision of starting idebenone was then made. At the last follow-up, an almost complete scotoma was observed in both eyes. No recovery of VA and VF was reported at 23 and 26 months follow up respectively in OD and OS.
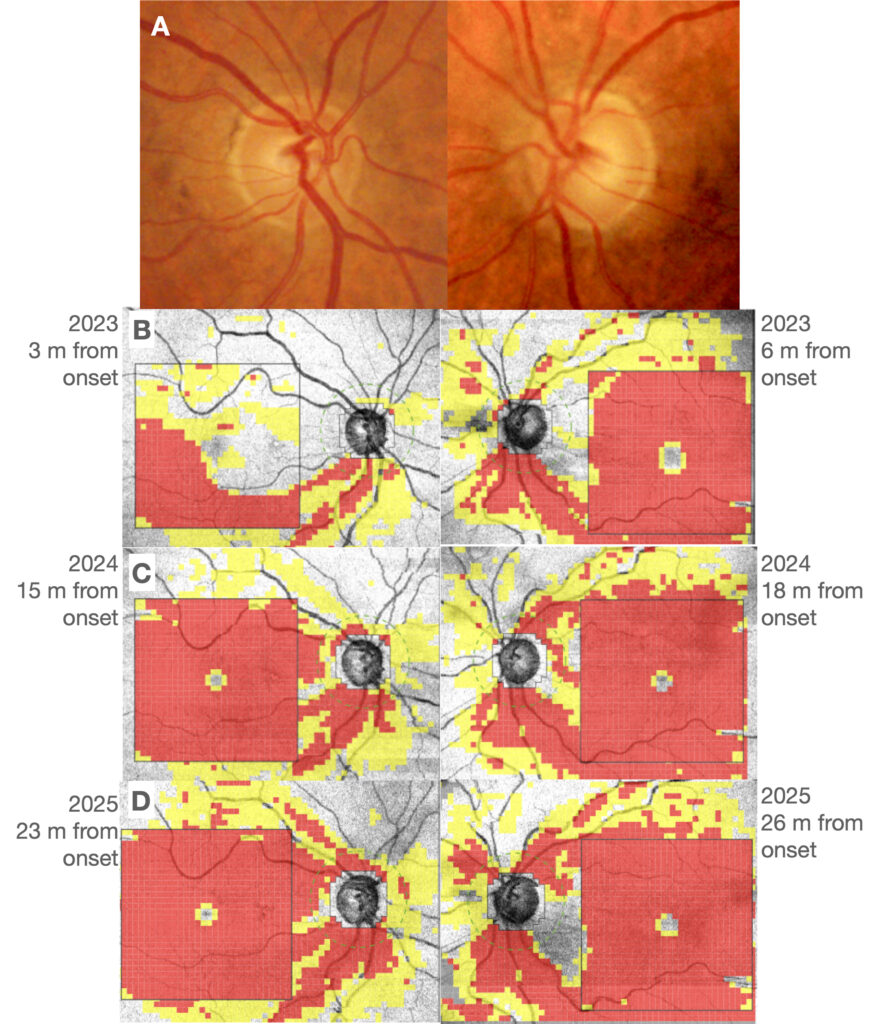
After few months, she reported poor vision in her left eye, followed by a decline in her right eye 3 months later. Despite the IOP was controlled, her visual acuity (VA) and VF continued to worsen, raising suspicion for a cause other than her glaucoma. At this time neuro-ophthalmologic evaluation her best corrected visual acuity (BCVA) was 3/10 in her right eye (OD) and counting fingers at 1 meter in the left eye (OS). IOP was within normal limits: 14 and 16 mmHg, respectively. Both optic nerve heads were small and with increased excavation (in particular OS, see figure 2A).
At the optical coherence tomography (OCT) scans of the optic nerve head, a deep damage of the retinal nerve fiber layer (RNLF) and macular ganglion cell layer (GCL) in the OS was observed, instead in the OD only a partial decrease in thickness was observed in the infero-temporal quadrant of GCL and inferior sector of RNFL (figure 2B).
Her medical history includes type 2 diabetes, hypertension, migraine, fibromyalgia, obstructive sleep apnea (OSAS) and Raynaud’s phenomenon. The patient was a non-smoker and had a body mass index of 20. Her family history was initially reported as non-contributory. A brain magnetic resonance imaging (MRI) revealed in 2023 an increase of multiple dot-like alterations in the supra-tentoral white matter, due to chronic vasculopathy, compared with previous exam of 10 years before. 24–hour blood pressure monitoring revealed highly variable systolic blood pressure during both day and night with multiple episodes of hypotension, with diastolic pressure values below 50 mmHg during both daytime and nighttime periods. Color Doppler imaging demonstrated reduced blood flow in the central retinal artery and short posterior ciliary arteries, more pronounced in the right eye. Polysomnography revealed obstructive sleep apnea (OSAS) treated with CPAP
At the follow-up, the patient demonstrated a worsening of visual impairment in the OD, with a residual visual acuity of 0.025 in her OD and 0.02 in the OS. IOP remained well-controlled in both eyes.
Figure 2. Optic nerve head at fundus examination and OCT of the optic nerve. (A) An increased and asymmetric excavation is observed in the left eye (OS) more than in the right eye (OD) with a slight pallor in this latter. (B) A marked defect of the retinal nerve fiber layer (RNFL) and a diffuse defect of the ganglion cell layer (GCL) is observed in the OS eye at baseline; in the OD the impairment is mostly observed in the inferior quadrant of the RNFL and GCL. (C) A progression of the defect in the RE is detected in the follow-up, with a diffuse involvement of the GCL and a thinning of the RNFL. The severe reduction of RNFL and GCL thickness in the OS is confirmed. (D) At last examination, 23 and 26 months from onset OCT analysis shows a progressive thinning of RNFL in both eyes.
The visual field progression trough the follow-ups is reported in figure 1 for both eyes.
During the same follow-up visit, it was clarified that a cousin (mother’s branch) had been diagnosed with Leber’s Hereditary Optic Neuropathy (LHON), a diagnosis consistent with the rapid progression observed in this case with a well-controlled IOP. Genetic testing subsequently confirmed the diagnosis of LHON (3460 mutation) in the patient. She was started on idebenone 900 mg daily and her glaucoma medication was adjusted in order to decrease IOP as much as possible excluding betablocker drops in order not avoid general hypotension. Moreover, she started OSAS treatment with CPAP and correct hypotension reducing antihypertensive therapy and introducing pentoxiphilline in order to increase ONH blood flow. At subsequent follow-ups, a progressive enlargement of the scotoma and a gradual thinning of both the RNFL and GCL were observed. At last follow up examination, 23 and 26 months from onset of visual loss, no recovery of VA and VF was reported and OCT analysis detected the progression of the damage in both eyes even in chronic stage (figure 2D).
In conclusion, this clinical case highlights the essential role of clinical history in establishing the diagnosis, as well as the importance of carefully assessing the relationship between function and structure in evaluating optic nerve damage. The diagnosis of LHON is sometimes very challenging, and when associated with glaucoma, it represents a severe condition that can lead to profound visual impairment even with a multimodal therapeutic approach.
How important is family history in hereditary optic nerve diseases?
Family history is critically important in the diagnosis and management of hereditary optic nerve diseases, in particular in LHON which is a mitochondrial maternally-inherited disease.1 In this case, the initial failure to identify a family history of LHON obscured the potential for a genetic cause for the patient’s rapid vision loss. Glaucoma management had successfully kept her intraocular pressure in a target range, but her vision continued to decline. The clue of a distant relative with LHON, which was revealed during a later consultation, was pivotal. It prompted genetic testing that ultimately led to the correct diagnosis. This case underscores that a thorough family history, including more distant relatives, is essential, especially when a patient’s symptoms are atypical or do not respond to standard treatment. It helps differentiate between common conditions and rarer hereditary disorders, allowing for timely and appropriate management. In the absence of typical LHON signs such as optic disc swelling or microangiopathy, it is essential to carefully assess the loss of the papillomacular bundle and the residual fibers typically preserved in glaucoma, up to the last area of vulnerability.2
What therapeutic strategy should be adopted in the coexistence of LHON and glaucoma?
The therapeutic strategy for a patient with coexisting LHON and glaucoma must address both conditions to preserve as much vision as possible. The two diseases can have an additive effect, accelerating damage to the optic nerve. Even if evidences are scarce, it is thought that the increased IOP due to glaucoma could trigger the onset of LHON.3
The primary goal remains to lower intraocular pressure (IOP) to slow the progression of glaucomatous optic nerve damage. In this patient, medication was initially adjusted from timolol/dorzolamide to dorzolamide only, while Latanoprost was continued. This choice was made to avoid any hypotensive damage to the optic nerve head, as observed in normal tension glaucoma.4 The goal is to find a regimen that effectively controls IOP without exacerbating any underlying vascular or perfusion issues. Prior to the onset of LHON, the patient underwent intensification of antihypertensive therapy (including alpha-blockers, calcium channel blockers, olmesartan medoxomil, and hydrochlorothiazide), which likely contributed to optic nerve hypoperfusion and was associated with progression of glaucomatous damage, particularly in the OS. Pentoxifylline, a rheologic facilitating oral drug, was prescribed to ease the blood flow inside the small capillaries of the optic nerve head, which may be beneficial given the patient’s diagnosis of Raynaud’s phenomenon and suspected systemic low blood pressure.5
At the same time, treatment for LHON focuses on addressing the mitochondrial dysfunction. The patient was started on oral idebenone, which acts as a mitochondrial antioxidant. It is the only approved oral treatment for LHON in some regions and can help stabilize or improve vision, particularly if initiated in the chronic phase and maintained for 24 months.6,7
Moreover, OSAS treatment should be continued in order to reduce oxidative stress during sleep.8
Furthermore, a lifestyle counseling is mandatory in this category of disease. The patient was advised to continue avoiding smoking and alcohol, as these can trigger or worsen LHON symptoms.
This case highlights the need for a multifaceted approach when multiple optic nerve pathologies are present. The management plan must be dynamic, adapting to the patient’s response to therapy and new clinical information to maximize the chances of visual preservation.
ECM
References
- Yu-Wai-Man, P. & Chinnery, P. F. Leber Hereditary Optic Neuropathy. Adam MP, Mirzaa GM, Pagon RA, al., Ed. GeneReviews® [Internet]. Seattle Univ. Washington, Seattle; 1993-2023.
- Hood, D. C. Improving our understanding, and detection, of glaucomatous damage: An approach based upon optical coherence tomography (OCT). Progress in Retinal and Eye Research (2017) doi:10.1016/j.preteyeres.2016.12.002.
- Thouin, A., Griffiths, P. G., Hudson, G., Chinnery, P. F. & Yu-Wai-Man, P. Raised Intraocular Pressure as a Potential Risk Factor for Visual Loss in Leber Hereditary Optic Neuropathy. PLoS One (2013) doi:10.1371/journal.pone.0063446.
- Killer, H. & Pircher, A. Normal tension glaucoma: review of current understanding and mechanisms of the pathogenesis. Eye (2018) doi:10.1038/s41433-018-0042-2.
- Ward, A. & Clissold, S. P. Pentoxifylline: A Review of its Pharmacodynamic and Pharmacokinetic Properties, and its Therapeutic Efficacy. Drugs (1987) doi:10.2165/00003495-198734010-00003.
- Amore, G. et al. Therapeutic Options in Hereditary Optic Neuropathies. Drugs (2021) doi:10.1007/s40265-020-01428-3.
- Yu-Wai-Man, P. et al. Therapeutic benefit of idebenone in patients with Leber hereditary optic neuropathy: The LEROS nonrandomized controlled trial. Cell Reports Med. (2024) doi:10.1016/j.xcrm.2024.101437.
- Meliante, P. G. et al. Molecular Pathology, Oxidative Stress, and Biomarkers in Obstructive Sleep Apnea. International Journal of Molecular Sciences (2023) doi:10.3390/ijms24065478.